
Assoc. Prof. Dr. Pınar Kadiroğulları
Assoc. Prof. Dr. Pınar Kadiroğulları is a specialist in obstetrics and gynecology. She specializes particularly in HPV treatment and cervical cancer prevention, providing holistic healthcare to her patients in the areas of pregnancy monitoring, genital aesthetics, and gynecological surgery.
By combining her academic background with clinical experience, she offers every patient an evidence-based, personalized treatment approach.

Myomectomy (Fibroid Surgery) is a modern treatment method that involves the surgical removal of benign tumors (myomas) developing in the uterus while preserving female fertility. In Turkey, myomas are observed in approximately 20-25% of women of reproductive age; a significant portion of these patients require surgical treatment due to their symptoms.
In modern gynecological surgical practice, a personalized surgical plan is created in line with the guidelines of the ACOG (American College of Obstetricians and Gynecologists) and the AAGL (American Association of Gynecologic Laparoscopists), taking into account the size, number, and location of the fibroids, as well as the patient’s desire for pregnancy. Assoc. Prof. Dr. Pınar Kadiroğulları offers minimally invasive and fertility-preserving treatment options to her patients with her expertise in advanced laparoscopic surgery at her clinic in Nişantaşı, Istanbul. You can also visit our Laparoscopic Surgery page for detailed information.
Information Note
Myomectomy should not be confused with the removal of the uterus (hysterectomy). Myomectomy is a fertility-preserving surgery where only the fibroids are removed and the uterus is preserved. With modern laparoscopic techniques, patients can be discharged within 1-2 days and can quickly return to their normal lives.
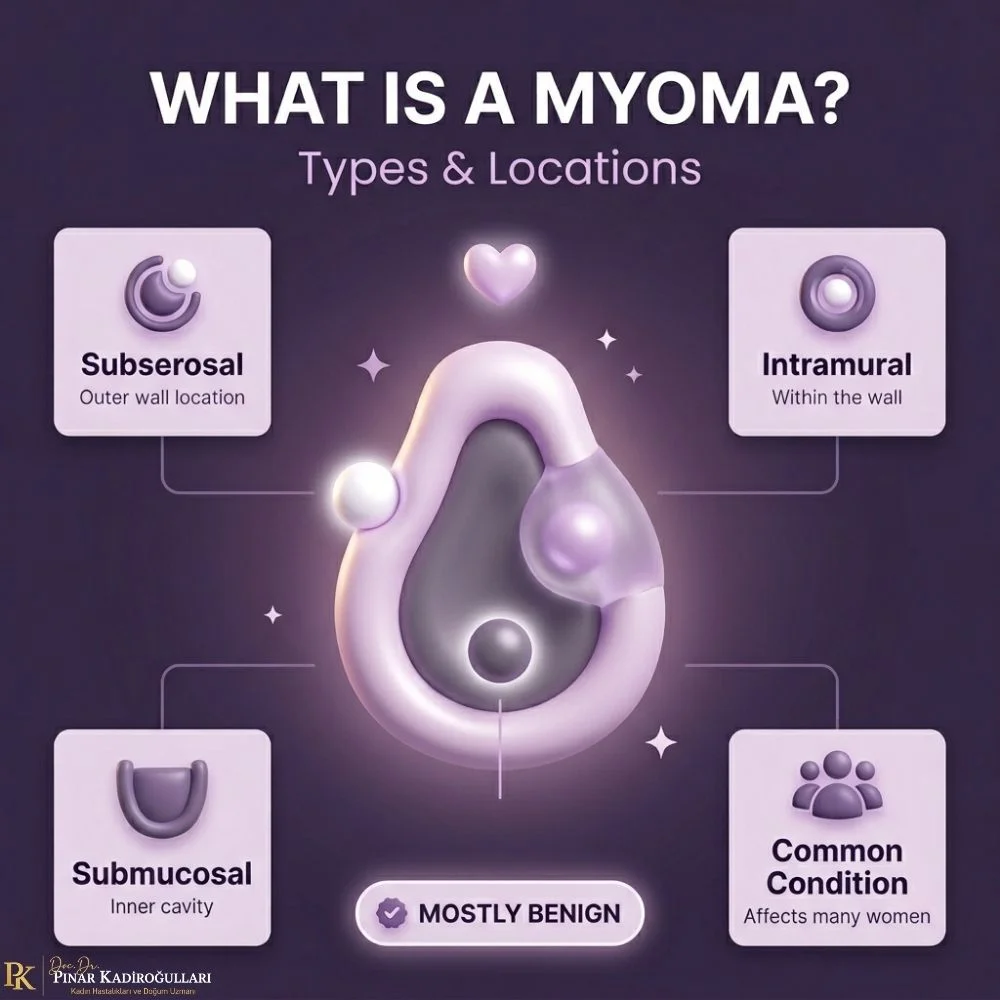
What is a Myoma and What are its Types?
Myoma (uterine leiomyoma) are benign tumors that develop from the muscle layer of the uterus (myometrium). These tumors, which are sensitive to estrogen and progesterone hormones, often appear in multiples and are more common in women of reproductive age.
Myomas are divided into three main types based on their location within the uterus, and the choice of surgical method is largely determined by this placement. The type of myoma is of critical importance when making a decision for myoma surgery:
1. Submucosal Myoma (Intrauterine): These are myomas located under the inner lining of the uterus (endometrium) that grow toward the uterine cavity. Removal via hysteroscopic myomectomy is ideal. This is the type that most frequently causes heavy menstrual bleeding and infertility.
2. Intramural Myoma (Within the Uterine Wall): These are myomas located within the muscle wall of the uterus. This is the most common type. Depending on the size, laparoscopic or open myomectomy is preferred.
3. Subserosal Myoma (Extrauterine): These are myomas that grow from the outer surface of the uterus toward the abdominal cavity. They can usually be easily removed via laparoscopy.
Important Information
Not all myomas require surgery. Small, asymptomatic myomas can be monitored with regular follow-ups. The surgical decision is made by considering the size, location, and number of myomas, as well as the patient’s age and desire for pregnancy. For detailed information on myoma disease, we will soon provide comprehensive information in our blog posts.
When is Myomectomy (Fibroid Surgery) Necessary?
The decision for myomectomy is based on the extent to which the patient’s symptoms affect their quality of life and the specific characteristics of the myoma. Small, asymptomatic (symptom-free) fibroids can be monitored with regular follow-ups. However, surgical treatment is recommended if the following conditions are present:
1. Clinical Symptoms
- Excessive and prolonged menstrual bleeding (menorrhagia)
- Intermenstrual bleeding (metrorrhagia)
- Bleeding leading to iron-deficiency anemia
- Chronic pelvic pain or a feeling of pressure
- Frequent urination or inability to urinate (bladder compression)
- Constipation or bowel compression symptoms
- Pain during sexual intercourse (dyspareunia)
- A palpable mass or swelling in the abdomen
2. Reproductive and Pregnancy Issues
- Infertility (especially with submucosal myomas)
- Recurrent pregnancy losses
- Uterine preparation before IVF (In Vitro Fertilization)
- Myomas posing a risk of preterm labor
- Large myomas leading to fetal malpresentation (positioning issues)
3. Structural Characteristics of the Myoma
- Rapidly growing myomas (especially after menopause)
- Myomas larger than 5 cm in size
- Presence of suspicion of malignancy (cancerous growth) in diagnosis
- Risk of torsion (twisting) in pedunculated myomas
- Submucosal myomas (those distorting the uterine cavity)
The Diagnostic Process
Myoma diagnosis is established via gynecological examination, transvaginal ultrasound, and MRI scans when necessary. Before a surgical decision is made, the size, number, location, and relationship of the myoma with other organs are evaluated in detail. This ensures the selection of the most appropriate surgical method.

Myomectomy (Fibroid Surgery) Methods
The choice of myomectomy method is determined by considering the type, size, number, and location of the fibroids. There are three primary approaches in modern gynecological surgery: hysteroscopic, laparoscopic, and open (laparotomy) myomectomy. Each method has its own specific indications, advantages, and limitations.
Method 1 – For Submucosal Myomas
Hysteroscopic Myomectomy
An incision-free surgical method where the myoma inside the uterus is removed by entering through the cervix.
- Indication: Submucosal myomas (extending into the uterine cavity).
- Duration: 30-60 minutes, general or spinal anesthesia.
- Discharge: Same day, return to normal life the next day.
- Advantage: No abdominal incision, rapid recovery, fertility-preserving.
- Limitation: Can only be applied to myomas located inside the uterine cavity.
Method 2 – Most Frequently Preferred
Laparoscopic Myomectomy (Closed Surgery)
A minimally invasive method where myomas are removed using a camera and instruments through 3-4 small incisions in the abdominal area.
- Indication: Subserosal, intramural, and mixed-location myomas.
- Duration: 1-3 hours, under general anesthesia.
- Discharge: 1-2 days, return to normal life within 1 week.
- Advantage: Small incisions, less pain, rapid recovery, excellent cosmetic result.
- Limitation: Careful planning is required for very large (>10cm) or numerous myomas.
Method 3 – For Special Cases
Abdominal (Open) Myomectomy (Laparotomy)
A traditional surgical method where myomas are removed through a single incision in the abdominal area.
- Indication: Very large or numerous intramural myomas, suspicion of malignancy.
- Duration: 1-3 hours, under general anesthesia.
- Discharge: 3-5 days, 4-6 weeks for full recovery.
- Advantage: Wide surgical field, suitable for many large myomas.
- Limitation: Longer recovery process, visible incision scar.

Recovery and Pregnancy After Myomectomy
The recovery process after myomectomy varies significantly depending on the surgical method used. With modern minimal invasive techniques, patients return to their daily lives much faster. As a fertility-preserving surgery, the chances of pregnancy after myomectomy are quite high.
Recovery Processes (By Method)
- Hysteroscopic myomectomy: Same-day discharge, return to normal life in 1-2 days.
- Laparoscopic myomectomy: Discharge in 1-2 days, light work for 1 week, full activity in 2-3 weeks.
- Open myomectomy: Discharge in 3-5 days, full recovery in 4-6 weeks.
Post-Operative Considerations
- First 24-48 hours: Mild bleeding and abdominal pain are normal and kept under control with painkillers.
- Heavy lifting is prohibited during the first week after surgery.
- Sexual intercourse: After 4-6 weeks (following a follow-up exam).
- Bathing: 1 day after hysteroscopic, 2-3 days after laparoscopic surgery.
- Regular walking increases blood circulation and supports healing.
- Watch for signs of wound infection: Consult a physician if there is fever, discharge, or severe pain.
Pregnancy After Myomectomy
- Waiting period for pregnancy: Varies between 3-12 months depending on the depth and number of myomas.
- After hysteroscopic: Pregnancy can be attempted 2-3 months later.
- After laparoscopic/open: 6-12 months (to allow the uterine wall to heal).
- The chance of pregnancy increases significantly after the removal of submucosal myomas.
- Myomectomy before IVF (In Vitro Fertilization) increases success rates.
- Mode of delivery: If deep incisions were made in the uterine wall, a Cesarean section is recommended.
⚠️ When to Consult Your Physician
- Fever above 38°C (100.4°F) or chills
- Redness, discharge, or foul odor at the wound site
- Severe pain that does not subside with painkillers
- Excessive or clotted vaginal bleeding
- Burning during urination or frequent urination
- Swelling, pain, or redness in the leg (thrombophlebitis)
- Sudden abdominal swelling or shortness of breath
Important Reminder
Myomectomy is a fertility-preserving surgery. The vast majority of patients experience a successful pregnancy after the operation. Our Infertility Treatment and High-Risk Pregnancy Follow-up pages also guide you through this process.
Frequently Asked Questions
Does Myomectomy Mean the Uterus is Removed?
No, the uterus is not removed during a myomectomy (fibroid surgery). Myomectomy is a fertility-preserving surgery where only the fibroids are removed while the uterus is preserved. The removal of the uterus is only performed in a different surgery called a hysterectomy. For all patients who wish to conceive, myomectomy is the preferred choice. With modern laparoscopic techniques, fibroids are successfully removed while uterine health is preserved.
How Long Does Laparoscopic Myomectomy Take?
Laparoscopic myomectomy typically takes between 1 and 3 hours. The duration varies depending on the number, size, and location of the fibroids. While a single small subserosal fibroid can be removed in 45-60 minutes, the duration may be longer for multiple or large intramural fibroids. Hysteroscopic myomectomy takes less time (30-60 minutes). Open surgery durations are similar to laparoscopic surgery, but the recovery time is longer.
When Can I Get Pregnant After Myomectomy?
The waiting period for pregnancy varies depending on the surgical method used. It is recommended to wait 2–3 months after hysteroscopic myomectomy and 6–12 months after laparoscopic or open myomectomy. This period is necessary for the uterine wall to heal sufficiently. In the case of an early pregnancy, the risk of uterine rupture may increase. Your doctor will determine a personalized waiting period for you based on the specific details of your surgery.
Is Normal (Vaginal) Birth Possible After Myomectomy?
The mode of delivery depends on the depth of the incision made in the uterine wall during myomectomy. Normal birth is possible after hysteroscopic fibroid removal. However, if a deep incision was made in the uterine muscle layer during laparoscopic or open myomectomy, a C-section is usually recommended due to the risk of uterine rupture during labor. The final decision will be made by your obstetrician after reviewing your surgery report.
Can Myomas Recur After Surgery?
The recurrence (re-formation) rate after myomectomy is approximately 15-30%. New myomas may develop again within 5-10 years. To reduce the risk of recurrence: accurate detection of all myomas before surgery, operation by an experienced surgeon, and regular gynecological check-ups after surgery are important. Since estrogen levels drop after menopause, the formation of new myomas is not expected. Regular follow-up and a healthy lifestyle minimize the risk to the greatest extent possible.
Our Treatments




Blog Yazılarımız
References
The medical content on this page has been prepared based on the current clinical guidelines and scientific publications of international and national authoritative organizations. Below, you can review the main PDF references cited and the academic publications of Assoc. Prof. Dr. Pınar Kadiroğulları.
ACOG Practice Bulletin No. 228: Management of Symptomatic Uterine Leiomyomas (Fibroids)
Author: American College of Obstetricians and Gynecologists (ACOG) | Publication: Obstet Gynecol 2021;137:e100-e115 | Source Type: International Clinical Practice Guideline (PubMed)
NICE NG88: Heavy Menstrual Bleeding and Uterine Fibroids — Assessment & Management
Author: National Institute for Health and Care Excellence (NICE) | Publication: NICE Guideline NG88 (2018, updated 2021) | Source Type: UK National Clinical Guideline (PDF)
Uterine Fibroid Management: A Comprehensive Review from Present to Future
Publication: Mol Hum Reprod 2018 | Source Type: Peer-Reviewed Review — Pathophysiology, Treatment Options, and Surgical Approaches to Fibroids (PubMed PMC, Full Text)
The Effect of Laparoscopic Myomectomy on Pregnancy Outcomes: A Systematic Review
Publication: Diagnostics (Basel) 2024 | Study: Meta-analysis of uterine rupture and fertility outcomes between 2008 and 2023 | Source Type: Peer-Reviewed Systematic Review (PubMed PMC, Full Text)
Comparison of Open and Laparoscopic Myomectomy: Patient-Reported Outcomes, Postoperative Morbidity, and Pregnancy Outcomes
Study: Retrospective analysis of 168 patients (2017-2023) | Publication: Archives of Gynecology and Obstetrics 2024 | Source Type: Peer-Reviewed Comparative Clinical Study (PubMed PMC, Full Text)
Fertility Outcomes After Robot-Assisted Laparoscopic Myomectomy: A 10-Year Experience
Study: 243 robot-assisted laparoscopic myomectomy cases | Publication: Cureus 2024 | Source Type: Peer-Reviewed Comprehensive Clinical Study (PubMed PMC, Full Text)
Laparoscopic Myomectomy and Pregnancy Outcomes: A Current Narrative Review
Publication: Cureus 2025 | Study: Postoperative pregnancy rates of 44-62%, uterine rupture <1% | Source Type: Peer-Reviewed Up-to-Date Review (PubMed PMC, Full Text)
⭐ Academic Publications by Assoc. Prof. Dr. Pınar Kadiroğulları on Uterine Surgery
Publications authored by the doctor in the field of uterine surgery, hysterectomy, and the development of surgical techniques
Abdominal Hysterectomy with a Uterine Manipulator: A Randomized Controlled Clinical Trial
Authors: Kıyak H, Karacan T, Özyürek ES, Türkgeldi LS, Kadiroğulları P, Seçkin KD | Publication: Journal of Investigative Surgery 2021;34(10):1052-1058 | Source Type: Randomized Controlled Clinical Trial (PubMed)
📍 This publication directly addresses hysterectomy, the most common surgery performed for fibroids — the effect of using a manipulator on vaginal structure during uterine surgery was evaluated through a randomized trial.
Modified Extraperitoneal Uterosacral Ligament Suspension: A 4-Clamp Technique After Vaginal Hysterectomy
Authors: Kadiroğulları P, Seçkin KD | Publication: Journal of Investigative Surgery 2019 | Source Type: Peer-Reviewed Clinical Research (PubMed)
Dermoid Tumor Coexisting with Endometrioma in a Single Ovary: A Case Report of the Laparoscopic Approach
Authors: Kıyak H, Kadiroğulları P, Karacan T, Seçkin KD, Karataş S | Publication: CRSLS – Journal of the Society of Laparoendoscopic Surgeons 2019 | Source Type: Laparoscopic Surgery Case Report
Important Note
The information on this page is intended for general informational purposes and does not replace individual medical advice. For personal questions regarding the diagnosis of fibroids, planning of myomectomy/hysterectomy, and your health, you should always consult your specialist gynecologist. The content of this page has been prepared by Assoc. Prof. Dr. Pınar Kadiroğulları in light of clinical experience and current scientific literature.
“Cutting-Edge Technology & Expert Experience”